
Download Lectures on Biostatistics (1971). Corrected and searchable version of Google books edition
Download review of Lectures on Biostatistics (THES, 1973).
Dangerous advice
A bizarre organisation called the NHS Trusts Association promotes not only homeopathy, but even wackier things like ‘crystal therapy’.
Read full entry on the original IMPROBABLE SCIENCE page.
An Edinburgh hospital is to supply aromatherapy on the NHS.
Read full entry on the original IMPROBABLE SCIENCE page.
The Amsterdam Medical Disciplinary Tribunal has struck off one doctor and suspended two others for their exclusive use of complementary treatments, resulting in the death of a woman.
Read full entry on the original IMPROBABLE SCIENCE page.
Trust Boots
Boots the Chemists (now Alliance Boots) is a very big business in the UK. There have 1,450 pharmacies in the UK and employ over 100,000 people.
I posted the item below a while ago, on the old Improbable Science page. I thought it deserved a bit more publicity, for the following reason. The quackometer has posted about Boots too,
I mentioned it during the debate with Felicity Lee at the British Pharmaceutical Conference (2007) (Ben Goldacre’s interview with Felicity Lee is a gem). After the talk I was approached by two heavies. Well, two men in dark suits anyway. It turned out that one was from Boots and the other from Alliance Pharmacies, now merged to form Boots Alliance. They seemed rather bothered by the fact that I’d criticised Boots, but were not entirely unreasonable. They claimed to be on the scientific side and said they’d investigate the matter. I wrote to the Boots man on 10 September, but got no reply, After a reminder on 29 October, I got this.
| Dear David Thank you for your email and reminder. We have investigated the points you raised in your blog. I was informed that it was an old leaflet and has not been reprinted (to my knowledge). However on a point of principle, I have raised the wider issue of clinical validity in my department. This will take its course through to the commercial/buying team. |
| Dear David Thank you for pointing this out. I’ve had a quick look and it is an educational website looking at all aspects of medicine and therapy, including alternative medicine. It is not a direct sales message to the public. I hope this helps |
Corporate Social Responsibility
Boots web site makes a big point about Corporate Social Responsibility (CSR)
“TRUST BOOTS
As you may have noticed, that’s the tagline which in 2005 we adopted as the sign-off to all our advertising. But it’s much more than just a slogan. It’s a concise statement of our entire corporate strategy. Our aim is to make Boots the world’s best health and beauty retailer, and we’re 100% clear that the unique trust in which we are held provides the key to achieving this. Which means, of course, that those two words are also the rationale for all our CSR activities. Everything we do that builds trust is good for our business; anything which could compromise it, a risk we can’t afford to take.”
Trust Boots to provide straight answers.
At one time. Boots were sufficiently ethical not to deal in homeopathy. But no longer.
When asked for evidence that the things they sell actually work, the Boots help desk is astonishingly coy, as related here (thanks to ebm-first.com for giving publicity to this report).
When Boots were asked about their ‘Alternatives Hayfever Relief Tablets’, the answer came, after some delay, “This is a homeopathic product, further information on homeopathic products is available from the Nelson company who make this
particular product for Boots. ” This company has been making homeopathic products for many years and
may well be able to help you further. You may also find general
information about homeopathic medicines in reference books in the public
library”. The email address that they gave me for Nelson’s did not work, and writing to another Nelson’s address produced no reply at all. Clearly any letter that contains the word “evidence” arouses suspicion and is simply deflected.
Dangerous advice from Boots: a small sting.
I have been into several Boots stores, sought out the most senior pharmacist that I can find, and asked them the following question. “I have a 5 year old son who has had diarrhoea for three days now. Please can you recommend a natural remedy”. The response was interesting. In every case but one, the pharmacist reached for a copy of the Boots pamphlet on homeopathy, and thumbed through it, while desperately, but unsuccessfuly, trying to retain an air of professional authority. Then one or another homeopathic treatment from the booklet was recommended. In only one case out of six did the pharmacist even mention the right answer (GP and rehydration). One pharmacist, who turned out to have qualified in Germany, was very insistent that homeopathic treatment was inappropriate and that I should should start rehydration and take the child to the GP. The other five, including one who had an impressive-looking badge saying “consultant pharmacist”, did not even mention rehydration.
Conclusion The education of the pharmacists was clearly insufficient for them to give reliable advice. On the contrary, their advice was downright dangerous.
Miseducation by Boots the chemists
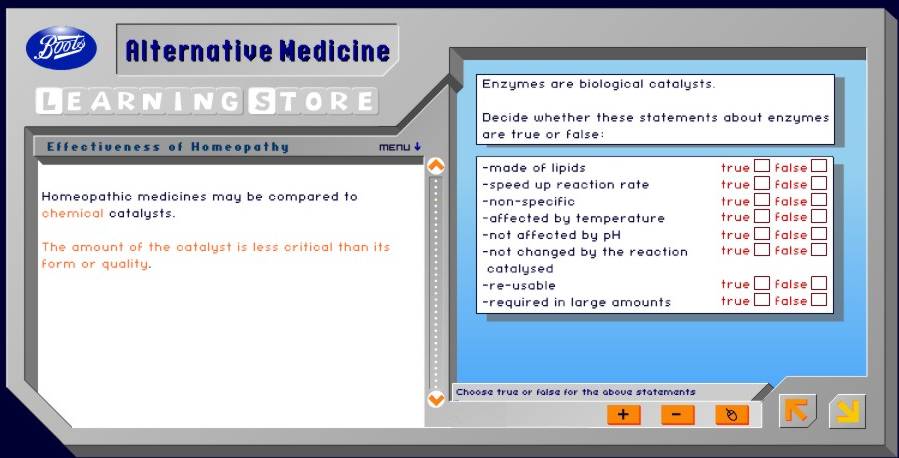
Boots also run an “educational” web site for children, the ‘Boots learning store’. Click on the section for ‘pupils’, and then ’16+’ and you find their education about alternative medicine (do their pharmacists do this course, I wonder?). The slide show that follows is an insult to human intelligence,
|
 |
Then follows a totally misleading slide about enzymes.
There is nothing wrong with the enzyme bit, but the analogy with homeopathy is baseless and misleading. Enzymes don’t work when there are no molecules present.
But in the next slide, enzymes and catalysts are forgotten anyway, This is how it works.

This meaningless mediaeval gobbledygook about ‘vital forces’ is being peddled as ‘education’ by the biggest retail pharmacy chain in the UK. What hope is there for kids?
But there is more. Now for the exam. If you click on the ‘teacher’ section you can download the students’ notes and the test. The ‘Student Notes’ include the following direct claim that homeopathy can cure diseases.

Now take the test, Here is question 1, and the answer.
I suppose that if the educators at Boots classify Hahnemann’s provings as a ‘clinical trial’ it goes a long way to explain the quality of their learning store, and the quality of the advice given by their pharmacists.
Boots Alternatives also sells a “snoring remedy”
The evidence for effectiveness of this herbal product is very dodgy, as described here earlier. This was an interesting saga that involved bad statistics, inappropriate controls and concealed financial interests. It eventually appeared on the BBC Radio 4 programme, You and Yours.
Postcript: “Nurses and pharmacists are to be given greater powers to prescribe drugs”
The foregoing history does not give one much confidence in the government’s latest money-saving wheeze. [BBC]
“The latest measures mean nurses and pharmacists will be able to prescribe treatments for more serious conditions such as heart disease and diabetes – traditionally the domain of GPs.
Health Secretary Patricia Hewitt said: “Nurse and pharmacist independent prescribing is a huge step forward in improving patient accessibility to medicines from highly skilled and well trained staff.”
And Chief Pharmaceutical Officer Dr Keith Ridge added: “For pharmacists, this is the dawn of a new era. It will help transform the public’s perception of pharmacy and the services they deliver to patients.”
This item was first posted on the original IMPROBABLE SCIENCE page.
Here is a link to a fascinating collection of essays that discuss “disease mongering”.
Read full entry on the original IMPROBABLE SCIENCE page.
In the discussion of magnets on the Badscience site, a Michael King says that 4ulcercare will be included in Part IX of the Drug Tariff because it meets the criteria of the Prescription Pricing Authority (PPA).
I presume this Michael King is Director of Planning and Corporate Affairs at the PPA, though he does not say so.
Michael King says
?There is no judgement offered about whether a product in the Drug Tariff
is more (or less) efficacious than any other, or the placebo effect.?
The criteria for inclusion in
Part IX of the Drug Tariff () include, in section 10 iii, ?They are cost
effective?
Will he please explain how a device can be cost-effective, if it is ineffective (relative to placebo)?
What the PPA says
Michael King has replied to my question by email (1 Mar 2006). He says
“The cost-effectiveness threshold for inclusion in the Drug Tariff is met if the ‘effectiveness’ of the device, as seen in data submitted by the manufacturer in support of the application, exceeds its cost to the NHS. ”
Sadly this is still ambiguous. It seems to suggest that that whatever data
are submitted by the manufacturer are taken at face value, without any attempt
to evaluate their quality. So I phoned King to ask if this was the case. He
was helpful, but he said that it was not the case. He told me that
the data were subject
to some sort of low level evaluation, short of the sort of evaluation that
NICE would do. This seems to contradict his earlier statement (above) that
inclusion in the Tariff implies no judgement about whether a device is better
than a placebo.
King said also that listing in the Tariff
“. . . is not a licensing decision nor a recommendation akin to the outcome of a NICE review”
The problem is, of course, that listing is seen as a recommendation by the public, by the Daily
Mail, and certainly by the manufacturer.
One thing, at least, is clear in this case. Whatever evaluation was done,
it was done very badly. But in order to try to find out exactly what evaluation
was done, and by whom, I’m having to resort to the Freedom of Information Act.
Watch this space.
What NICE says
Fraser Woodward (Communications Manager, National Institute for Health and Clinical Excellence (NICE)) writes as follows.
“The test of “cost effectiveness” applied by the PPA when determining whether or not a device should go on the tariff is very different to the way cost effectiviness is assessed by NICE”
That is pretty obvious, but how is the public meant to know that, when they hear that the NHS has declared a treatment to be ‘cost-effective’, that statement can mean two entirely different things according to which part of the bureaucracy the statement comes from?
Several of the people who contributed to, and/or appeared in, the BBC2 series on alternative medicine, have complained that they were treated “like marionettesâ€, and that the programme was sensationalised and uncritical,
Read full entry on the original IMPROBABLE SCIENCE page.
The Office of Fair Trading has taken Magno-Pulse Ltd to the High Court after they refused to stop what the OFT regards, quit rightly, as misleading advertising. This is the company whose magnets have just been approved by the PPA for prescription on the NHS!
Read full entry on the original IMPROBABLE SCIENCE page.
In the discussion of magnets on the Badscience site, a Michael King says that 4ulcercare will be included in Part IX of the Drug Tariff because it meets the criteria of the Prescription Pricing Authority (PPA)
.
I presume this Michael King is Director of Planning and Corporate Affairs at the PPA, though he does not say so.
Michael King says
?There is no judgement offered about whether a product in the Drug Tariff
is more (or less) efficacious than any other, or the placebo effect.?
The criteria for inclusion in
Part IX of the Drug Tariff () include, in section 10 iii, ?They are cost
effective?
Will he please explain how a device can be cost-effective, if it is ineffective (relative to placebo)?
What the PPA says
Michael King has replied to my question by email (1 Mar 2006). He says
“The cost-effectiveness threshold for inclusion in the Drug Tariff is met if the ‘effectiveness’ of the device, as seen in data submitted by the manufacturer in support of the application, exceeds its cost to the NHS. ”
Sadly this is still ambiguous. It seems to suggest that that whatever data
are submitted by the manufacturer are taken at face value, without any attempt
to evaluate their quality. So I phoned King to ask if this was the case. He
was helpful, but he said that it was not the case. He told me that
the data were subject
to some sort of low level evaluation, short of the sort of evaluation that
NICE would do. This seems to contradict his earlier statement (above) that
inclusion in the Tariff implies no judgement about whether a device is better
than a placebo.
King said also that listing in the Tariff
“. . . is not a licensing decision nor a recommendation akin to the outcome of a NICE review”
The problem is, of course, that listing is seen as a recommendation by the public, by the Daily
Mail, and certainly by the manufacturer.
One thing, at least, is clear in this case. Whatever evaluation was done,
it was done very badly. But in order to try to find out exactly what evaluation
was done, and by whom, I’m having to resort to the Freedom of Information Act.
Watch this space.
What NICE says
Fraser Woodward (Communications Manager, National Institute for Health and Clinical Excellence (NICE)) writes as follows.
“The test of “cost effectiveness” applied by the PPA when determining whether or not a device should go on the tariff is very different to the way cost effectiviness is assessed by NICE”
That is pretty obvious, but how is the public meant to know that, when they hear that the NHS has declared a treatment to be ‘cost-effective’, that statement can mean two entirely different things according to which part of the bureaucracy the statement comes from?
Emails in my possession show that the Chiron Clinic is able to decide that nutritional supplements are needed for leg ulcers on the basis of an email (as well as magnets of course).
Read full entry on the original IMPROBABLE SCIENCE page.
This is a slightly modified version of some thoughts from the old improbable science page, where they formed part of the review of a BBC2 series on alternative medicine. It has been moved to the new blog because of the comments posted here.
Evolution of plants
Plants didn’t evolve for our benefit. Natural selection ensures that plants, like every other living thing, evolve in a way that maximises their own chance of survival. To ensure that, plants should be as toxic as possible to anything that might eat them. The more harm a plant does to humans, the better its chance of survival. It is sheer luck that some of the toxic principles evolved by plants occasionally turn out to be useful.
| Memo to: The members of the Kansas Board of Education From: God Re: Your decision to eliminate the teaching of evolution as science Thank you for your support. Much obliged. Now, go forth and multiply. Beget many children. And yea, your children shall beget children. And their children shall beget children, and their children’s children after them. And in time the genes that made you such pinheads will be eliminated through natural selection. Because that is how it works.’ . . . ; By Gene Weingarten, Washington Post Staff Writer. Saturday, August 14, 1999; Page C01 |
Naturalness
Here are some products of nature. That doesn’t mean they are good for you.
Lead, uranium, radon, arsenic, thallium, strychnine, cyanide (in Sorghum and Prunus species), Stinging nettles, poison ivy, yew, deadly nightshade, castor beans (ricin), tobacco, curare, foxglove, fly agaric, (muscarine), death cap (amanita phalloides), . . ..
Foxgloves, heart failure and biological standardisation
Here is a bit of relevant pharmacological history.
The 24th edition of Martindale’s Extra Pharmacopoeia (1958) describes Digitalis Leaf (B.P., I.P.), also known as Digit. Fol.; Digitalis; Foxglove Leaf; Feuille de Digitale; Fingerhutblatt; Hoja de digital.
| It was defined as “the dried leaves of Digitalis purpurea (Scrophulariaceae).”At that time it was sometimes prescribed as Prepared Digitalis (BP), which is “Digitalis leaf reduced to powder, no part being rejected, and biologically assayed the strength being stated in units per g. For therapeutic purposes it must be adjusted to contain 10 units in 1 g.”Sometimes foxglove leaf was prescribed as Tincture of Digitalis (B.P., I.P.). “It may be made from unstandardised leaf, the tincture being subsequently biologically assayed, or it may be made from prepared digitalis, using a quantity containing 1000 units per litre, by percolation or maceration, with alcohol (70 %). It contains 1 unit per ml. I.P. allows also 1 unit per g. Dose: 0.3 to 1 ml. (5 to 15 minims). ” |
 |
Although these preparations are now totally defunct, they were still better than the sort of thing that is now advocated by herbalists. Why? They were better because they were standardised.
Foxglove leaves contain several chemical compunds that are useful in certain forms of hear failure. But the margin of safety is quite low. Take a bit too much and it kills you not cures you. One batch of foxglove leaves will contain different amounts of active compounds from the last batch, and that endangered patients.
From the 1930s onwards, pharmacologists developed methods of biological assay that overcame this problem. An international
standard digitalis leaf sample was established. Every new batch had to be assayed against this standard, and diluted to a fixed level of biological activity. This ensured that each batch of digitalis powder had the same biological potency as the last batch. It was a great pharmacological advance in its time. But of course it did involve the use of animals for the biological assay.
All this was solved when the active principles were purified from the foxglove leaves. There was no longer any need to uses animals for biological assays. The right amount of pure digoxin or digitoxin could be weighed out.
Fortunately herbalists are not allowed to prescribe anything as potentially dangerous as digitalis. But in general herbalists are happy to use pre-1930, unstandardised plant extracts.
I can think of no case in which there is the slightest reason to think that the mixture of chemicals in the plant is any better than the purified active principles. Of course there could be such cases of synergy. But that is just idle speculation.
No surprise there then, because idle speculation is the stuff of alternative medicine. It’s a great deal easier than making the effort to find out what works, and probably more lucrative too.
This entry has been transferred from the old IMPROBABLE SCIENCE page..
The Open University is a great institution. Its first vice-chancellor was Walter Laing Macdonald Perry . Before he took that job, he was professor of Pharmacology in Edinburgh (and one of my Ph.D. supervisors). He must be turning in his grave at the new OU course, K221 – Perspectives on Complementary and Alternative Medicine .
The course description sounds harmless enough, ” This course provides an accessible but rigorous introduction to complementary and alternative approaches to health.”. But just how rigorous is it? The game is given away when you see that the “experts” seem mostly to be true believers, people who make their living from alternative medicine. How can such people be expected to the merits of the systems of beliefs
that are the basis of their livelihood? It is rather like having a rigorous discussion about the existence of god in which all the course tutors are priests. Take some examples.
The bit about Testing Therapies is by Elaine Weatherley-Jones, She is in clinical practice as a homeopath. And as you might expect the three pages on the web about ‘testing therapies’ are highly partisan and selective. Try these quotations.
“In homeopathy, the vital force is said to be responsible for maintaining health, combating disease by recruiting the body’s natural tendency to cure itself. In the homeopathy model, disease occurs when the vital force is not working efficiently to keep the balance of health.”
“. . . in The Manual of Conventional Medicine for Alternative Practitioners : “The essence of alternative medical thought is that there is a vitalistic principle behind and encompassing any physical object”, explaining that “vitalistic” means that there are “objects which are non-physical in part or whole”. The vital
force of homeopathy and qi of TCM are non-physical – it’s impossible to see them, no matter how powerful an electron microscope was used. Qi and the vital force are ideas that are put forward to explain how the body heals itself.”
“Vital forces”? Which century are we living in? If this were offered as social studies, perhaps it would not matter, but the Open University is offering this course as part of a B.Sc. degree. Then we get the usual weasel words about the impossiblity of testing empirically whether alternative medicines (CAM) produce an effect, regardless of how they work. That is the important question. After all we are pretty vague about how some conventional drugs work. In a mind-boggling passage we are told that it is impossible to test CAM against a placebo, but quite possible to test CAM against an orthodox treatment.
It seems, incidentally, that the author’s grasp of pharmacology, and of the literature, is a bit weak. “. . . when Belon and his colleagues reported research in 2004 in the journal Inflammation Research , they showed that ultra-high dilutions of histamines (which are proteins involved in allergic reactions and causes, for example, inflammation of the breathing tubes in asthma) are active in influencing human cell activity. ”
Histamine (there is only one), is not a protein? This is meant to be a university course! Belon, of course, is a committed homeopath. This passage conveniently ignores the fact that his experiments have been repeated at least twice by respectable scientists, and they find no such effect. Surprisingly enough, they find that no drug gives no response. Amazingly, it seems that the OU would have us think otherwise.
The rest of the course seems to be much the same. The dispassionate expert on Herbal medicine is a herbal practitioner who makes his living from it, and is just as uncritical as one might expect in that circumstance. Unlike Weatherley–Jones, though, he does come clean (more or less) about the lack of evidence as to efficacy of herbal remedies (though that evidently does not deter him from practising the subject).
The “expert” on acupuncture , Rosey Grandage, is a bit more interesting on the history of her subject, but is every bit as committed to CAM as the others. She works at the University of Westminster as course leader of the Diploma in Qi Gong Tuina and also lectures on the BSc Acupuncture course. ” Rosey practices as a physiotherapist, acupuncturist and tuina practitioner in West London”. Hardly an unbiased observer. “ . . . it is this growing popularity which answers the question of whether acupuncture has a place in the modern world.”
Is it not obvious that the long persistence, and popularity, of an idea cannot possibly be used as an index of truth? One merely has to think of the long-persistent and popular ideas about the ‘one true god’. Clearly at most one of these can be true. The history of medicine is replete with popular and persistent ideas that turned out to be untrue. Take nux vomica . For hundreds of years conventional medicine regarded strychnine as a ‘tonic’. That persisted right up to the 1950s. But it became apparent that it just did not work, and strychnine, and the very word ‘tonic’, vanished from the vocabulary of rational medical people. You
won’t be surprised to find, though, that is still widely touted by fraudulent herbalists.
It could be argued that the course is intended as sociology rather than science, though the course description does not say so, and the course can count towards a BSc. Even as sociology though, it would seem better if the viewpoint of the tutors was rather broader.
The course books
I have now obtained copies of the three course books that were used for K221last year. They are indeed written largely as sociology not as science. But it is a highly biased sort of sociology, as one might have expected from the commitments of the authors. Although there are occasional references to lack of evidence, this does not seem to deter the authors from their relentless pursuit of the ‘integration’ of CAM into medical practice.
A superficial reading by a naive student might give an impression that the books are a “rigorous introduction to CAM”. The more sophisticated student is likely to see them as subtle, even insidious, propaganda. I won’t claim to have read all three books. Opening almost any page makes obvious their not-very-hidden agenda.
Here are a few examples from CAM: Structures and Safeguards (eds. Geraldine Lee–Treweek, Tom Heller, Hilary MacQueen, Julie Stone and Sue Spurr).
Chapter 5 (Homeopathy: principles practice and controversies) contains a ludicrously biased account ot the affair of Jacques Benveniste (see here and here ). There is no mention of the fact that his results were disproved at the time, and at least twice since, I know of only one group that has claimed similar results, and that group, like Benveniste’s, contained committed homeopaths. There is no mention of Beneveniste’s two Ignobel prizes. There is no mention of the fact that after he left France in disgrace, he went on to claim that the properties of the alleged memory of water could be sent by email, a claim so absurd that it has not persisted even within CAM.
This chapter uses the standard CAM trick of redefining the word efficacy. Rather than its usual meaning of having an effect greater than placebo, it is conveniently redefined to mean, roughly, ‘patients say they feel better’,
“Although the issue of whether or how homeopathic remedies ‘work’ is a major bone of contention for medical scientists, the fact that they perceive that the remedies do work makes it attractive to many orthodox medical practitioners.”
So that’s OK then. Don’t trouble yourself with what’s true.
Chapter 1 of ‘CAM: Structures and Safeguards’ has the title “Knowledge, names, fraud and trust”, and is by Geralidine Lee-Treweek. It is a fine example of relativism -almost post-modernist in style. This is a discussion of knowledge in which the words ‘true’ and ‘false’ barely appear. The student who lent me
the book has scribbled in the margin “If it is not true and right –then it is not knowledge”. Pass the student, fail the tutor . (in fairness, it has to be pointed out that the student passed with distinction, despite her scepticism.)
So does Open University course K221 really give you a “rigorous introduction to complementary and alternative approaches to health. ” No it seems that it does not. Here are some more reasons.
A student who has successfully completed course K221 has told me that
- “It was very anti-science and anti-orthodoxy in places”
- “I had several ‘discussions’ with her [OU tutor] in our online tutor group, some about her anti-vaccination stance and the fact that she was happy to give homeopathic anti-malarials to travellers.”
The argument that homeopaths at least do no harm ( see above ) seems to be destroyed by their advocacy of policies that will lead to more children getting measles, and which will contribute to the spread of malaria. There is an ultimate irony in OU tutors preaching against vaccination. Walter Perry, the first vice-chancellor of the OU, before he was my supervisor in Edinburgh, had been Director of Biological Standards at the Medical Research Council’s labs. In that job he had responsibility for introduction of polio vaccine in UK. That effectively eliminated the scourge of polio.
This is not what a real university should be doing, as part of a B.Sc. degree.
An article on the death of homeopathy, There has been long enough to get evidence, but it is not there.
Read full entry on the original IMPROBABLE SCIENCE page.
On 21 November, 2005, Dr David Spence appeared on the BBC’s Today Programme. He was being interviewed about a report that, he said, provided evidence for the effectiveness of homeopathy. In fact it does nothing of the sort.
Dr Spence’s paper was published in the Journal of Alternative and Complementary Medicine. It is not really research at all. They simply asked 6544 patients who had had homeopathic treatment whether they felt better or not. Half the patients (50.7%) said they were ‘better’ ot ‘much better’. A further 20% said they were ‘slightly better’. The patients who had homeopathic treatment were not compared with anything whatsoever!
This is reported in a straighforward way. What is quite ludicrous is the stated conclusion of the paper:
“The study results show that homeopathic treatment is a valuable intervention”.
It is obvious that there is not the slightest reason to attribute the answers given by patients to the fact that they had been given homeopathic treatment. That would be the crudest form of post hoc ergo propter hoc error. It does not even show that the homeopathic treatment was producing a placebo effect.
Papers like this do not add to human knowledge, they detract from it. By reverting to pre-enlightment forms of argument, they mislead rather than enlighten. To make matters worse, this work was done at public expense, by the Directorate of Homeopathic Medicine, United Bristol Healthcare, National Health Service Trust, Bristol, United Kingdom.
What on earth is a respectable hospital and medical school, like those in Bristol, wasting money with this sort of mediaeval hindrance to medical knowledge? We are truly living in an age of delusions.
Download the paper and see for yourself [ Spence DS, Thompson EA, Barron SJ. J Altern Complement Med. 2005, 11, 793-8. pdf file, 74 kb].
The Daily Telegraph recently published two reports about acupuncture. One said it worked. The other said it didn’t work. Needle cure effect ‘is not all in the mind’ By Catriona Davies, starts
Acupuncture has a genuine ability to relieve pain, scientists have found.
The other report was
Doubt cast on needle therapy for migraine By Nic Fleming, Health Correspondent, starts
Acupuncture is no better at reducing migraines than fake treatment, researchers say today.
A study involving more than 300 patients found the healing method did reduce headaches, but only by the same amount as placing needles at non-acupuncture points.
Unfortunately the Daily Telegraph‘s reporters did nothing to help the confused reader. No comment was made on the apparent contradiction. In this particular case, there is an obvious explanation.
The first (favourable) article was said to be published in Nature, though in fact it was published in Neuroimage (Pariente J., White P., Frackowiak , Richard S. J. & Lewith G. Neuroimage, 25. 1161 – 1167, 2005). Presumably the reporter had picked it up from a rather uncritical synopsis on the news site, nature.com. It was conducted on 14 patients with painful osteoarthritis. Contrary to the first line of the Telegraph‘s report (“Acupuncture has a genuine ability to relieve pain”), the work did not measure pain at all. In fact the summary of the paper says
“The three interventions, all of which were sub-optimal acupuncture treatment, did not modify the patient’s pain.”
What the paper actually did was to use positron emission tomography (PET) to measure ‘activation’ of certain parts of the brain when needles were inserted. Some parts were activated more by having acupuncture needles piercing ths body than by ‘stage-dagger’ needles which retracted and did not pierce the body. I have no criticism of these findings: my purpose here is to explore the apparent contradiction between this trial and another.
The second, unfavourable, report was of a much bigger study, 302 patients with migraine headaches. It was published by Linde et al. (Journal of the American Medical Association. 2005 293(17):2118-25). This study concluded
“Acupuncture was no more effective than sham acupuncture in reducing migraine headaches although both interventions were more effective than a waiting list control. ”
These two studies were on quite different conditions, used different methods, and very different numbers of patients. But suppose we take them at face value, are they not contradictory? No, not necessarily, because they used quite different sorts of control group.
The study that was reported as showing that acupuncture worked compared patients that had real acupuncture with patients who had treatment with “stage dagger” needles that appeared to pierce the skin but did not.
The study that was reported as showing that acupuncture did not work (Linde et al.) used a different sort of control group, acupuncture needles that pierced the skin but were inserted in the wrong places (as defined by the ‘principles’ of acupuncturists). No difference was found between ‘real acupuncture’ and control.
There is nothing incompatible about these two studies if one adopts the view that piercing the skin with a needle can produce a physiological response that makes the patient feel that other sorts of pain are less painful, but that it does not matter where the skin is pierced. The latter hypothesis means, of course, that all talk about “meridians”` and “energy flow” that acupuncturists use, is no more than mumbo jumbo.
Dr Lewith is quoted as saying, of the negative study, “This is a badly conceived study that just adds more confusion to the debate because it uses non-site specific acupuncture as a control.” Quite on the contrary, the Linde study seems more interesting to me, because it unveils the mumbo jumbo of meridians (at least for the particular points used in this study). Dr Lewith may find this conclusion unpalatable, but it is the obvious implication of this pair of studies.
Another study confirms that the principles of acupuncture are nonsense
A trial by Melchart and colleagues on 270 patients shows conclusively that acupuncture can indeed produce amelioration of tension-type headache when compared with no treatment, BUT the relief is produced whether or not needles are inserted at ‘acupuncture points’. Very similar results were found with ‘superficial needling at non-acupuncture points’. British Medical Journal, 15 August 2005. Yet again it is shown that the mumbo-jumbo of meridians and magic points is nonsense. Yet again, that is a good reason why universities cannot be expected to train acupuncturists. Our business is to minimise mumbo-jumbo, not to propagate it.